Health Information Sharing as Feminist Rhetorical Work: Rethinking Power, Individuality, and Simplicity in Women and Their Bodies1

Health Information Sharing as Feminist Rhetorical Work: Rethinking Power, Individuality, and Simplicity in Women and Their Bodies1
Peitho Volume 21 Issue 3 Summer 2019
Author(s): Sarah Singer
Abstract: This article contends that health information sharing is an urgent concern for feminist rhetoricians. As we transition from using manuals to using internet platforms to find health information, users are prompted to share their data. How do these platforms persuade women and other vulnerable patients to share their health data—and at what personal cost? Building on work by Robert Johnson and Jordynn Jack, I argue that a feminist rhetorical approach to user-centered, data sharing technologies involves three key principles: power, simplicity, and individuality. To demonstrate, I engage a user-rhetorician perspective to rhetorically analyze Women and Their Bodies and MyLymeData, a current health information sharing platform. I conclude by imagining what truly user-centered versions of health information sharing platforms might look like and considering directions for future research.
Tags: Chronic Lyme, health information sharing, Lyme disease, sharing economy, user-centered technology“In the previous sections to this course, we have discussed the problems women face in their encounter with our medical system. We have been given inadequate and often incorrect information on how our bodies function. We can’t get birth control, so thousands of us die each year from illegal abortions. Childbirth is often a tarrying and inhumane experience. These problems are not mistakes, they are results of a system which is designed to make profits, maintain a professional elite, and treat certain sick people, rather than deal with the problems of human beings and their illnesses.”
– Women and Their Bodies (179, emphasis added)
The authors of Women and Their Bodies (WATB), the earliest version of Our Bodies, Ourselves (OBOS), cautioned readers about the growing power of the “healthcare economy” long before such a term was in circulation. Although the authors encourage users to further their health education, they warn them to be wary of particular organizations, insurance companies, and, ironically, doctors. The authors characterize Ortho and Tampax as “capitalist organizationsp” [sic] that “[push] their own products for profit” (5), and they contend that Planned Parenthood “pushes population control and birth control pills” (5). The authors alert users to insurance companies’ goals and practices, noting that healthcare “will be the nation’s largest industry” by 1975 (182). They explain that doctors earn additional profits from Medicare’s “usual and customary” billing system (186), and they examine evidence from a range of sources to reveal how the privatization of hospitals prevents low- and middle-income patients from seeking care (186).
But the authors could not have anticipated that health information is the primary capital of the twenty-first century healthcare economy. Today, in an age of chronic, ambiguous, and contested health problems, sharing health data—which includes culling anecdotes, doctor’s names, medical tests, and validated and experimental treatments—is a necessary strategy for gathering information. Patients with these challenging conditions rely on data sharing for multiple reasons. Primarily, traditional doctors and data from clinical studies have not cured their health problems. After years of living with ambiguous symptoms and paying for expensive, ineffective treatments, these patients remain ill. They do not want to pursue additional treatments without clear justification. They worry that consulting with too many medical providers may be seen as suspect and thus wish to pursue healthcare selectively. Accordingly, these patients seek out others’ health data via social media, patient advocacy groups, nonprofit organizations, “fringe” healthcare providers, and data sharing apps and repositories, all of which offer more capacious discussions of chronic, ambiguous, and contested health conditions and user-generated data (Singer).2
However, processing user-generated patient data can be confusing, especially for patients who face dire health circumstances. Women, in particular, are vulnerable yet empowered in their search for adequate healthcare and health information. In Tasha Dubriwny’s words, they are forced to “grapple with and make active decisions” based on a range sources with ambiguous credentials, including websites, magazines, and advertisements (6). These sources are made more confusing by “[n]eoliberal marketing strategies,” which “have effectively blurred the line between medical research and marking of pharmaceutical drugs and illnesses” (147). As part of this dynamic, when patients review other patients’ data, they often feel compelled to share their own. Lori Beth De Hertogh notes that new “interactive features” in online health spaces, such as discussion boards, prompt users to “collectively produce and share health-related content” (“Feminist Digital” 486). Clearly, patients stand to benefit from reviewing other patients’ health data, but what do they gain from sharing their own health data? And, perhaps most importantly, how are patients persuaded to share their health data—and at what personal cost?
As patients shift away from a manual-centered health information sharing system, in which texts such as OBOS were central, they will be forced to seek out other validated sources and make choices about sharing their own health data. Because OBOS and other trusted print sources are no longer being updated, patients must learn to navigate a confusing digital terrain replete with persuasive appeals. As they decide which apps, websites, and platforms are worthy of their attention (and data), Robert Johnson’s framework for classifying user-centered versus user-friendly technology remains a helpful guide. Building on Johnson’s framework and Jordynn Jack’s embodied feminist rhetorical approach to examining mobile technologies, I argue that a feminist rhetorical approach to user-centered technologies involves three key principles: power, simplicity, and individuality. To demonstrate, I first show how the principles work by rhetorically analyzing WATB, which I assert is a truly user-centered text. Next, I show how a current health information sharing platform, MyLymeData (MLD), employs similar rhetorics of user-centeredness but does not yet achieve the same goals for transformative access as WATB. Even when MLD and other technologies appear to be system-disrupting and claim to “help a user to manipulate parts of the system, negotiate the system, or change the system even in a small, local way,” they still require users to agree to their restrictive terms and conditions and submit their data in exchange for access (Seigel 74). I examine WATB and MLD as a user-rhetorician, drawing on my experiences as a patient and a scholar to reveal the complexities of health information sharing. I conclude by imagining what truly user-centered versions of health information sharing platforms might look like and considering directions for future research.
From Manual to Digital: User-Centered Technology and Women and Their Bodies
As Marika Seigel (2013) and Sarah Hallenbeck (2015) have shown, there have long been manuals about women and their bodies, most of which circumscribed their agency and opportunities for engagement. Although it is celebrated for many innovations, Susan Wells argues that WATB (published in 1970) was the first manual that prompted women to “investigate their own bodies directly” (185). Wells and Seigel clarify that WATB was unusual for this reason and others. Seigel argues that manuals often “assume uncritical acceptance of the technologies and processes about which they instruct the reader” and take for granted “an expert-notice relationship between the rhetor and reader” (32). However, like many contemporary social media platforms, blogs, and digital health information repositories, WATB framed users as experts—or at least equals—and engaged them by invoking their knowledge and experiences. Similarly, the authors created the manual by combining scientific and medical research with their own experiences with healthcare. They “decided on the topics collectively” and “were doing research and writing that were about us and for us” (3). The authors’ horizontal workflow, which included undertaking a “dynamic” process of writing, “g[iving] support and helpful criticisms to each other,” and rewriting, meant that the users were integral and the knowledge was crowdsourced (3).
In turn, WATB and newer digital health sharing platforms have three key things in common: the centrality of the user, the focus on user expertise, and the collection of crowdsourced information. In Robert Johnson’s book, User-Centered Technology: A Rhetorical Theory for Computers and Other Mundane Artifacts, he theorizes the role of the user and considers how users “unwittingly surrender knowledge and power due to our lack of reflection on our mundane interactions with technology” (10). Johnson defines users quite simply: as “the audiences of technology” (xv). User-centered technologies, he argues, offer users an opportunity to be “active participants” in the “negotiated process of technology design, development, and use” (32, emphasis original). Seigel contends that WATB, the first version of OBOS, is truly user-centered and, accordingly, provides a model of a system-disrupting technology. These technologies allow users transformative access, or the ability to change the technology in ways that benefit them personally as well as others in the system. In other words, the authors of WATB hoped that users would not simply learn to identify their body parts, but also to have orgasms, discover their sexual proclivities, advocate for themselves in clinical environments, create additional content, teach the content to other women, and reform the healthcare system to make it less sexist, racist, and classist. Seigel focuses on the chapter on pregnancy, which aims to “[disrupt] the user’s functional engagement with the components (or subsystems) of the healthcare system” (74) and, as such, “overwhelmingly focuses on questions of definition and evaluation” (76). In the remainder of this section, I extend Seigel’s work by reading across the text to consider how the authors invoke power, simplicity, and individuality, aiming to empower users to help themselves and radically reform the healthcare system. From there, I compare WATB with MLD, a contemporary health information sharing website, to pose questions about the challenges of creating transformative user access in the current age of health information sharing.
From its instantiation, the structure, organization, and content of WATB aimed to enable transformative user access. WATB is merely 193 pages long and divided into twelve sections. The authors envision the manual to be a “course” in women’s health. Using this frame, the authors encourage users to draw on their own expertise and offer “more deliberative than prescriptive” instructions for examining women’s bodies (Seigel 81). In an effort to provide transformative user access, many sections of WATB focus on patients’ power (and lack thereof in most cases).3 In the introduction, the authors discuss how the users were “an integral, participatory force in the process of writing” (Johnson 31). There is a long section about the iterative writing, drafting, and revision process, which involved groups of women from across the Boston area. The authors note that the text is “not final” (3) and “not static” (3), recognizing that it “should grow and include other topics” based on users’ needs (4).
To further empower users, the authors urge them to use the manual “as a tool” for prompting “discussion and action, which allows for new ideas and change” in an effort to ensure that users’ needs are met (4). Similarly, the content of the manual centers users’ ambitious needs and goals: to “act together on our collective knowledge to change the health care system for women and for all people” (4). Whether the authors are discussing the “capitalist medical care system,” which they emphasize is “no more dedicated to improving the people’s health than can General Motors become dedicated to improving people’s public transportation,” or the doctor-patient relationship, they aim to empower users to understand their personal power in relation to the institutions that govern U.S. healthcare (8).
Moreover, the authors offer simple, straightforward information using a simple, straightforward approach. They streamline complex medical terminology and information so that it is easy to understand, but they do not undermine users in the process. The authors critique the “pseudoscientific jargon” that allows doctors to “set themselves off from other people” (8) by offering relevant medical terminology alongside relatable analogies. In the “Women, Medicine, and Capitalism” section, for instance, the authors discuss female sex organs and suggest methods and reasons for self-investigating them. Specifically, they offer a short, friendly description of how a reader can palpate her cervix:
“You can touch your own cervix; it feels like a large nipple with a small dimple in its center, extending from the top part of the vagina way towards the back. The uterus changes position during the menstrual cycle, so where you feel the cervix one day may be slightly different from where it will be next! The entrance into the uterus through the cervix is very small, about the diameter of a very thin straw. This is the little dimple that you feel in the middle of the ‘nipple.'” (12)
The description is conversational rather than technical, clearly oriented towards the user population: women who were self-aware but unfamiliar with their reproductive anatomy. Readers are addressed in second person. They “can” touch their vaginas—they are able to and empowered to if they wish. The description of the cervix as a “large nipple with a small dimple in the center” and the entrance to the uterus as “a very thin straw” are colloquial and would have been easily understood by users at the time. The addition of an exclamation point signals the surprising joy that can be found in learning about one’s body, which is an affordance of self-investigation that benefits users personally. Later in that section, the authors note, “We emphasize that you take a mirror and examine yourself. Touch yourself, smell yourself, even taste your own secretions. After all, you are your body and you are not obscene” (14). Here, the language is more directive, but the authors know that most users have internalized overwhelming shame about their bodies, particularly their vaginas, and they must prompt users to work through this shame to become more educated and, thus, be more empowered as they make decisions about their healthcare (Adams). By offering accessible yet explicit instructions for investigating their sex organs, the authors show how a plain language approach to healthcare instruction can be simple without being reductive.
Despite their effort to simplify information and provide general knowledge, the authors still manage to emphasize users’ individuality. Throughout the “course,” the authors highlight the importance of individuality by providing a range of personal stories from contributors and encouraging users to figure out what works for them specifically. The authors explain that the paper on sexuality, in particular, includes many personal stories “because we felt that our own voices, our own histories rang the clearest and truest and helped us reclaim the mysterious topic of sexuality as familiar and ours” (16). These personal stories, or vignettes, are a few sentences long and present a wide variety of experiences, including instances of sexual pleasure, confusion, and violence. Even fraught topics such as masturbation (23) and sexual fantasies (30) are covered comprehensively. Moreover, with each vignette, the authors honor the individual’s story and reemphasize their focus on the individuality of the user. After the vignettes about masturbation, to take one example, the authors note, “If you have never masturbated, don’t feel like you are confined to these techniques. Finding what you like to do is what it’s all about” (23, emphasis original). This multifaceted understanding of individuality remains a central focus throughout the “course.” As the authors emphasize, “By talking to each other, taking support from each other, we can set our own standards which will bear the mark of sanity and individuality” (18). Such notes make it clear that the authors do not simply want users to replicate other users’ techniques or experiences, but instead to pay attention to their own individual needs to improve their wellbeing.
Later on, the authors emphasize repeatedly that the manual is not merely a how-to guide for pleasing women; instead, it is a course designed for personal and collective empowerment. They address “any men who happen to read” the course directly, noting that it is not a “marriage manual” (37). Instead of experimenting with the advice offered by the course, the authors implore men to “change [their] behavior” and “start doing half the housework” (37). This is yet another instance in which the authors reinforce the importance of individuality and using the manual to discover themselves and their needs, not to please others nor find a universal approach to doing so.
In all, WATB functions as both a manifesto and a manual, offering critiques of the capitalist, “pay-as-you-die” (7) healthcare system alongside accessible instructions for how users might explore their own bodies and personally benefit from reading the text. Unlike WATB, which aimed to convince users to self-investigate as a way to counter the “corporate capitalist entities” (7) that make up our healthcare system, contemporary data-sharing technologies are created and sustained by the “new medical-industrial complex” (Relman 963). These apps, websites, and health data sharing platforms often deploy a rhetoric of user-centeredness that is eerily similar to that of WATB, emphasizing qualities such as power, simplicity, and individuality. However, while these platforms claim to help patients, they may also profit in various ways from collecting their health data. Whether or not they are selling the data to interested companies, health data collection platforms may seek to gain political power or influence, advocate for certain treatments over others, and more. Additionally, as Marissa J. Doshi and other scholars show, data sharing may have unanticipated consequences (197). In a study of over 100 of the most popular Google Play apps, researchers found that more than 70% shared users’ data with outside sources, such as Amazon and Google (Grundy et al.). The study found that data sharing in health apps is “routine,” and that some forms of unauthorized data collection are considered “legitimate business practice[s]” despite issues with consent, privacy, and ethics (n.p.).
In what follows, I offer a case study of MLD, a nonprofit health data collection platform for Lyme disease patients. By charting the struggles of Chronic Lyme disease patients and others who struggle with chronic, contested, and ambiguous illnesses, I consider why these patients are motivated to share their health data and the questions and concerns they may have as they make data-sharing decisions.
Lyme Disease and MyLymeData
Lyme disease is just one example of the many chronic, ambiguous, and contested conditions from which Americans increasingly suffer. Lyme disease is a common condition that comes bacterium transmitted to humans when they are bitten by infected deer ticks. Theoretically, Lyme disease is simple to diagnose and treat, and recovery should begin as soon as it is treated. According to the most recent clinical guidelines, patients who are diagnosed quickly after their initial infection and treated with antibiotics for fourteen to twenty-one days are expected to recover completely (Wormser et al.). However, there is no consensus in the medical community about how to diagnose or treat persistent, ambiguous Lyme disease symptoms, which impact 10-20% of patients (Rebman et al.). Many people refer to these persistent symptoms as Chronic Lyme Disease, but term is hotly contested in the medical community. Thus, patients may suffer for years from so-called “subjective symptoms,” such as joint pain, fatigue, and brain fog, waiting in vain for a diagnosis, which, as medical anthropologist Mara Buchbinder notes, may be “the fundamental explanatory act in medicine” (9). Since Chronic Lyme patients face challenges with receiving a correct diagnosis (Hirsch et al.) and may “undergo multiple diagnostic tests while being seen by many health care professionals from numerous subspecialties, thus extending the time to diagnosis” (Drew and Hewitt 23), they seek out information in the interim.
With delays in diagnosis and few long-term solutions, Chronic Lyme disease patients are forced to consult shared health data on blogs, “Lyme literate” doctor’s websites, patient advocacy websites, nonprofit organizations, and social media platforms in an effort to get well (Singer 161). Patients and their allies face a difficult crossroads. Since there are no simple cures for Lyme disease, patients are left with one option: they can take comfort in sharing their pain, their stories, and their data to prevent others from experiencing the same suffering. For many patients, these sharing platforms are critical. For instance, users may compile their health data in apps to help them track symptoms, identify trends, chart a history of treatments. Most importantly, patients’ participation in data sharing does not (ostensibly) adversely affect their ability to obtain healthcare, render them “noncompliant,” nor interfere with their current treatment plans. In turn, ill individuals may see sharing their health information as less risky than not sharing their information. So, with few other choices, they share their data and examine other patients’ shared data.
When I first came across MLD, the primary health information sharing platform for Lyme disease, I felt energized for the first time in months. It seemed like website authors knew me and my Lyme disease story and were speaking directly to me. I was immediately drawn to the text in the center of the homepage, which reads, “IMAGINE A WORLD where people with Lyme disease are diagnosed and treated correctly and go back to living their lives” (“Home”; see Fig. 1; emphasis original). I have imagined this world for eleven years, since I was diagnosed with Lyme disease in November 2009. I am one of the 300,000 or more people who are diagnosed with Lyme disease each year (“Data and Surveillance”), and I am one of the 10-20% of patients who are affected by long-term “subjective symptoms” (Rebman et al.).

Fig. 1. MLD homepage, 19 February 2019, https://mylymedata.org/. Screenshot by author.
Reading on, MLD tells me, “YOU CAN BE PART OF MAKING THIS HAPPEN” (emphasis original) and implores me to “Add your Lyme data to MyLymeData to help find a cure for Lyme disease” (“Home”). Throughout the years, I have suffered significantly. I would do almost anything to prevent others from the same pain: negotiating with well-intentioned but disbelieving doctors, taking drugs that cause intolerable side effects, spending thousands of dollars on medical tests, and sleeping away their youth. I have worried about my treatments, which sometimes caused more harm than good. I have taken conventional medications, such as antibiotics, anti-inflammatories, and biologics, and paired them with elimination diets, exercise, and other complementary therapies. I have dreamed about “living” my life and recovering from Lyme disease. I have felt so powerless over my own body—which doctors tell me is my responsibility to control—and it is exhilarating to think that I can use my experience to help others. And, perhaps more importantly, to help myself. The next paragraphs explain the goals of the website, but I have already clicked the bright orange “Count Me In!” button to sign up. This is the moment I have been waiting for: I can be “counted on” to share my experiences of suffering, which, more importantly, will finally “count” for something, towards something better.
MLD’s immediate goal is quickly producing research that improves Lyme disease diagnosis and treatment processes. In a recent letter to Peitho, the Principal Investigator elaborated on MLD’s history and mission:
“MyLymeData is one of the very few patient-driven research projects in the nation. The registry is a project of LymeDisease.org, which was founded in 1989 as a grass-roots organization. Over 80% of the members of the board of directors of LymeDisease.org are patients or have family with Lyme disease and the Principal Investigator is a patient who suffered from chronic Lyme disease. Hence, MyLymeData is run by patients, and holds patient interests at the center. The funding for MyLymeData is exclusively from individual donors or individual foundations. We do not sell data to pharma, commercial industry interests, or any other entity. We are a trusted community based data steward for vetting researchers, data use and re-use, and ensuring that data is used to benefit Lyme disease patients.” (Johnson, “Letter”; emphasis original)
To achieve this goal, MLD implores users to share their health data, which the MLD leadership team studies and shares with others at their discretion. “User [s]ubmitted [c]ontent,” as noted in the Terms & Conditions, “may be available for viewing by other registered users or toLDo-approved4 affiliates, service providers or other business partners of LymeDisease.org as de-identifiable data only, for research, statistical, study, and evaluation purposes” (Terms & Conditions). Because MLD is a project of LymeDisease.org, a nonprofit that has been advocating for Lyme disease patients since 1989, users likely believe that the organization’s key “principles”—patient empowerment, participation, and self-determination”—inform its selection process for data sharing (“Who We Are”). However, as a user-rhetorician, it seems as though users are an “integral, participatory force” in MLD’s data collection process (Johnson 30) but also “inevitably ancillary” when it comes to circulating and publishing the data (27). MLD cannot conduct research without users’ health data, but users do not appear to be leaders in the research development nor publication processes.
In the next section, I consider how MLD employs similar rhetorics of power, simplicity, and individuality as WATB. While the platform aims to support Lyme disease patients, my interpretation of the website’s content suggests that it does not yet offer transformative user access. As I will suggest, a truly patient-powered data sharing tool would ensure users transformative access to information as well as tangible benefits from sharing their data.
Power
MLD’s use of the term “patient-powered” is its most significant rhetoric of user-centeredness. The term appears on nearly every page of the website. On a page titled “Patient Powered,” the term is defined more specifically: “MyLymeData expects to gather more data about Lyme disease than any research study has done before and build a patient-centered research community. That’s what patient-powered research is about!” Further down the page, the authors note that “New technology allows patients to take the lead” and “MyLymeData lets patients lead the way to help find a cure” (“Patient Powered”). As a user-rhetorician, the idea of “patient-powered” research is very exciting to me because it seems like a bottom-up, rather than a top-down, approach to gathering data. To me, “patient-power” suggests that patients are leaders in the data collection, use, and sharing processes. Traditional clinical trials are “patient-powered” in the sense that researchers gather and process patients’ data, from which they discern results and make recommendations for future research, treatments, and protocols. Patients like me do not have power beyond choosing to participate. However, the idea that MLD is “patient-powered” makes me think that typical users like me are at the helm of making important research and publication decisions.
After reading more closely, though, it becomes clear that MLD users cannot share any of the data they find on MLD without explicit permission. The Terms & Conditions page outlines the “[a]llowable [a]ctivities” for users: “users shall not disclose, post, publish, display, or transmit any of the Website content, without the written consent of LymeDisease.org.” In order to do anything publicly with the “user-submitted content,” including “downloading,” “modifying,” or “distributing” the data, users must “secure all necessary rights and permissions” (Terms & Conditions). As a user-rhetorician, it might be helpful for me to look at other users’ data to see, for instance, which medications they are using to treat their Chronic Lyme disease. However, telling my illness story has always been central to my healing process. Whether I am sharing it in private groups on social media sites, blogging about it, or writing about it as part of my academic work, my personal and scholarly mission is bringing attention to the plethora of information available to health seekers and how they make decisions about that information. I draw on my personal experiences with illness to help students, academics, and community members understand why some people rely on “bad” sources, try dangerous treatments, and thwart traditional medical research. Even though the official purpose of MLD is to “allow individuals, families and medical and research providers to register certain information on the Website’s registry database” (Terms & Conditions), the rhetoric of “patient-power” that permeates the website makes me feel like the platform wants to help me directly.
Most of the MLD webpages are directive and friendly, promoting the benefits of “patient-power” in Lyme disease research. Regardless of what any other page says, though, I am bound by MLD’s terms and conditions. While the majority of the website is replete with invitational, bold colors and graphics, the Terms & Conditions page seems typically system-centered. It includes large blocks of text and does not match the same infographic style as the rest of the website. In my work as a patient and as a rhetorician, comparing, analyzing, and amplifying recent research about Lyme disease is crucial. While many health information sharing platforms do not allow even partial access to disaggregated, deidentified data, MLD does not offer me transformative access if I cannot share the information without a review and approval process.
Moreover, as a user-rhetorician, I trust the leaders at MLD to make careful choices about who is allowed to access my data. However, I was not permitted to gain researcher-level access to the MLD data, which made me wonder about the selection process. When I contacted MLD in 2017 about their work and asked for a copy of their survey questions, the Primary Investigator offered to talk with me but wrote that it was “unlikely that [she] would provide [me] with a copy of [the MLD] survey as it is confidential and proprietary” (Johnson, “Dissertation”). Ultimately, we were unable to connect. I was surprised that MLD seemed opposed to allowing a graduate student, especially one who is deeply invested in seeking equitable treatment for Lyme disease patients, to review their survey. While there may be valid reasons why MLD chose not to provide me with researcher-level access to their data, the process made me—a user-rhetorician—question how their policies were different from for-profit health information sharing platforms. To whom do they give access and why? Again, I was reminded that even though I contributed my data, I cannot share it without permission, even in service of conducting additional research to further the cause.
As I continue to review MLD as a user-rhetorician, I am struck by some of the paradoxes of the “patient-powered” research process. It seems like patients power the website by sharing their data, but patients have little power in what happens to their data once they share it. It seems like the idea of health information sharing is powerful enough to harm patients, but MLD employs powerful rhetorics to persuade users to share their data with minimal acknowledgement of the potential consequences. Even though MLD does not sell patients’ data, other organizations and companies do. I am surprised that there is not greater acknowledgement of the problems with data misuse and breaches, especially since MLD is a nonprofit and does not benefit financially from patient’s data. There are also other, more subtle places where I am reminded that I am a regular user—that my “patient-power” is serving MLD rather than me specifically. On the “About MyLymeData” page, the MLD authors note, “After the first one, we will send you additional surveys (about quarterly) asking additional questions and tracking your progress. We will let you know what we discover.” The we-you-we pattern here illuminates a persuasive hierarchy: MLD is the organizing and authoritative power that propels me into action, but they cannot have power without me. Although users can view the data, only high-level authorities make decisions about developing, analyzing, and circulating it for broader audiences. While the LymeDisease.org advisory board members are primarily Lyme disease patients and healthcare experts, they are also business leaders, authors, and members of other advisory boards (“Board of Directors”). At press time, they hail solely from California and Utah. It is hard to imagine that they fully understand my experiences as Lyme disease patient from the east coast and that I would agree with their choices about collecting and publishing MLD’s data. This hierarchy is very different from WATB, in which users are encouraged to adapt the course to meet their personal and specific community’s needs. Again, I was struck by the differences between MLD’s discussion of “patient-power” the discussion of power in WATB. Instead of empowering users to become part of the health information sharing process to help themselves and help reform the healthcare system, MLD’s rhetoric struck me as a classic example of neoliberalism at work, in which patients are conscripted into sharing their data and are not compensated for their efforts.
Individuality
In addition to the focus on “patient-power,” the MLD authors deploy ostensibly user-centered rhetoric that acknowledges users’ individuality. MLD’s focus on individuals and individuality is primarily constructed through two key phrases, which appear on multiple pages of the website: “Count me in!” and “Can one make a difference?” (see Fig. 1). These phrases appear to be user-centered, but they ultimately work to persuade patients to contribute their data to MLD, which may not necessary help them directly. This is vastly different from the authors’ inclusion of personal stories and perspectives in WATB. The phrases, “Count me in!” and “Can one make a difference?,” emphasize that individual voices are not merely important but integral to finding a cure for Lyme disease.
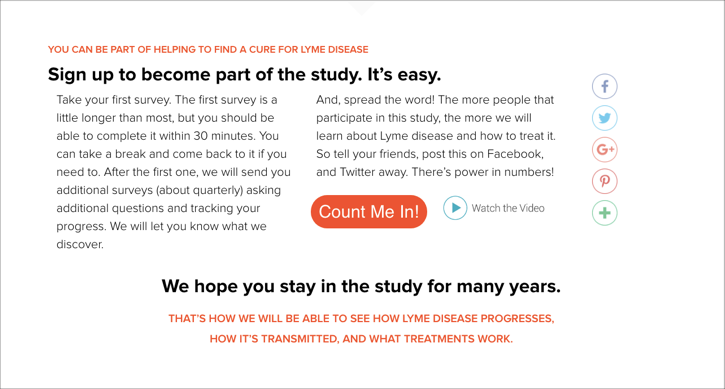
Fig. 2. “Count Me In!” button on the “About MyLymeData” page, 19 February 2019, https://www.lymedisease.org/mylymedata/national-study-chronic-lyme-disease/. Screenshot by author.
The phrase “count me in!” has multiple meanings, particularly for Lyme disease patients like me (see Fig. 2). Although researchers in fields such as entomology, public health, rheumatology, and infectious diseases are studying Lyme disease, there have been only a few clinical trials for patients with Chronic Lyme (Turk et al.). Clinical trials for Lyme disease often have strict inclusion criteria, requiring multiple positive tests and the presence of a bull’s eye rash. I, personally, have not qualified to participate in any clinical trials despite all of the documentation verifying that I tested positive for Lyme disease. Since interested patients like me are unable to participate in these clinical trials, we are excited about other opportunities to advance research. More than that, I want to be counted. After years of doctors questioning my pain and evading answers about my prognosis, I want to move forward knowing that others will not have to suffer in the same ways that I did. The language of “counting” honors individuals’ identities, stories, and experiences, especially Lyme disease patients who do not “count” in other settings. This user-centered rhetoric invites users to contribute their data and authorizes them to share diverse experiences. It’s important to note, however, that once I am “counted,” I am still not authorized to share any information I learned from MLD without permission.
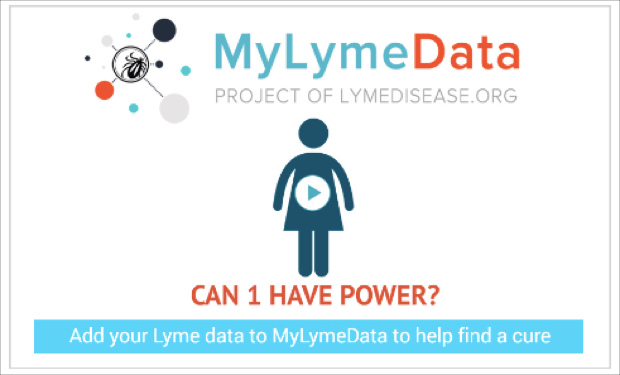
Fig. 3. “Can 1 Have Power?” video slide, 19 February 2019, https://www.lymedisease.org/mylymedata/videos/. Screenshot by author.
The second phrase—“one can make a difference”—suggests that that I, personally, can help create new scientific knowledge about Lyme disease. This phrase is primarily presented in the 1:28 minute video, “Can 1 Have Power?,” which is featured at the top of the MLD “Home” page as well as on the “Videos” page (see Fig. 3).This video begins by asking “Can one person have power?” and tells me, “If you have Lyme Disease, YOU’RE NOT ALONE” (“MyLymeData Videos,” emphasis original). This statement resonates with me. For the first five years especially, I felt isolated because of my illness. Each time a friend complained that I cancelled plans due to illness, asked why my fatigue could not be cured with a nap, or wondered how I could be so young and so sick, it reaffirmed that chronic illness was destroying my social life. The video goes on to introduce “big data,” which is framed as a “new kind of research” that combines individual experiences to learn more about Lyme disease. As a user-rhetorician, I’m surprised by the simplistic definition that is offered: big data “is a big deal” and “allows you to fight Lyme disease with your own health information.” Starting in 2013, so-called “big data” has been critiqued in highly respected publications such as The New York Times, Scientific American, Time Magazine, Newsweek, and The Atlantic. The video goes on to explain, “When researchers study lots and lots of health data from you and thousands of others living with Lyme disease, they can see patterns. And those patterns could lead to better understanding, treatments, or even a cure for Lyme disease.” I can appreciate this idea, but it also makes me wonder: What will be missed by looking at Lyme disease experiences through a big data lens? I am worried about what “big data” means at MLD and how they take care to preserve the texture and individuality of people’s stories. It seems like users do not need to understand anything about science or “big data” to feel agented (or perhaps more significantly, obligated) to contribute to Lyme disease research. The video concludes, “It’s within your power to change the future, starting right now. Add your Lyme data to my Lyme data, and help find a cure for Lyme Disease.” At this point, it almost seems unethical for me not to contribute my data and increase the seemingly exponential power of MLD’s big data project.
After watching the video, I can understand how big data might be a useful tool for researchers, but I am not yet sure how it will help me individually. To me, it makes sense that gathering and analyzing large quantities of data and searching for patterns can provide new insight about Lyme disease. Perhaps when this research is published it will make a difference for me, but in the interim, I am not sure what this research method offers. It seems like another example of how the MLD appears to center users but has designed the platform to serve their own interests. On the “About MyLymeData” page, MLD suggests that “big data” is what makes their study so simple and easy. They cite three easily comprehensible benefits of big data research: it “provide[s] lots of information,” “uses very broad entry criteria,” and “examines treatments used in the real world.” And yet there is no acknowledgement that big data requires patient labor and creates an exclusive sharing economy, which economist Chris J. Martin defines as the exchange of knowledge, tools, skills, or other information that is primarily “driven by digital technologies” (152). As it plays out on MLD, users must become members and share their data in order to gain access to the platform’s data repository. Although sharing economies may lead to “a more sustainable form of consumption,” they may also be rhetorically “reframed by regime actors as purely an economic opportunity” (Martin 149). In other words, sharing economies may reinforce system-centered practices and technologies. Estee Beck notes that sharing can allow for “reciprocity, trust, and…altruism,” but her work suggests that it can also have a “dark side” that involves “capitalistic exploits of unpaid labor of its users” (38). I am left wondering about how the sharing economy shapes MLD’s big data project. It is difficult to compare it to WATB, which does not require users to share their data to gain access to the information and has clear benefits for individual users.
Simplicity
As I think more about MLD and how its rhetoric agents me—as an individual—to share my story and my data, I cannot help but think about how easy the website makes it to do so. MLD employs a rhetoric of simplicity and goes to great lengths to make it possible for users to contribute, but it prompts me to ask: How could contributing my personal health data be so simple? What am I missing? The language of simplicity, ease, and speed contradicts the rhetoric of complexity that typically undergirds scientific work.
These concepts appear on most pages of the MLD website, beginning on the “Home” page. The authors contend, “Our patient surveys draw over 9,000 responses! We’ll use the information provided by patients to help figure out how to prevent and treat all stages of Lyme disease. It’s that simple” (emphasis added). Similarly, the “About the Study” page urges users to “Sign up to become part of the study. It’s easy” (emphasis added). It is strange to think about the MLD surveys as “simple,” since there are multiple surveys that ask hundreds of questions about users’ experiences with Lyme disease. For me, answering all of the questions might require me to look back at my medical records, speak with my range of medical specialists, and “fact check” key symptoms and dates with my partner. Furthermore, “simply” taking the survey may require a relatively high level of medical literacy that goes beyond the scope of some users’ comprehension. In turn, the repetition of this language seems to detract from the complicated issues at stake, such as data security.
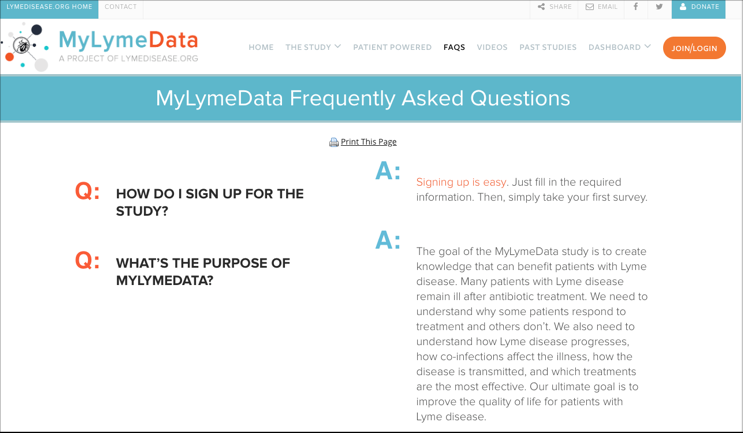
Fig. 4. MLD FAQ page, 19 February 2019, https://www.lymedisease.org/mylymedata/faqs/. Screenshot by author.
With these issues in mind, I turn to the FAQ page in search of answers. As a user-rhetorician, I see FAQ pages as essential to my understanding of how a platform works and what I can expect if I choose to engage with it. By nature, FAQ pages appear to be user-centered because they seem to anticipate users’ questions and concerns. In this case, however, the MLD FAQ page appears to prioritize its organizational needs over me, the user. Users are immediately confronted with this concept of simplicity, starting with the first question: “How do I sign up for the study?” (see Fig. 4). Rhetorically, the content managers have chosen to put this information first because they want users to pay the most attention to it. The answer to this question, accordingly, is “Signing up is easy. Just fill in the required information. Then, simply take your first survey” (“FAQ,” emphasis added). Two FAQ questions in particular focus on the language of simplicity. In the answer to Question 7, the content creators report that “If you are of legal age (18 years old in most states), simply sign up” (emphasis original). Similarly, in question 9, which is about privacy, the answer notes that if I get uncomfortable, “[w]ith few exceptions, [I] can simply skip questions [I] prefer not to answer” and that if I decide to withdraw from the registry, I can “[s]imply contact the registry and all of [my] data will be removed from the database” (“FAQ,” emphasis added). The repetition of the word “simply” here is notable because without signing up and taking a survey, it is unclear, exactly, how easy it is for participants to skip questions and revoke their data.
Some of the questions that I need answered, such as “How will my data be used?” and “What about privacy?” are buried in the middle of the FAQ list, which does not have numbers or bullet points. For me to read the list, I am forced to either control+F search for this information or skim through large blocks of small text. The second-to-last questions—“Is there IRB approval for the study?” and “Who can I contact if I have questions about the study?”—may be the most important of all, but again, they are buried in the FAQ list and are not organized in a user-centered way. The questions themselves are easy to read, but they generally focus on how I can contribute to MLD rather than how MLD will protect me, my story, and my data. For example, Question 5 reads, “What is expected of me?” and Question 7 reads, “How can I participate?” These questions prioritize me, the user, by employing first-person language, but the answers repeat information that is available throughout the website rather than sharing additional details.
After I review the FAQs, I find that I still have other questions, so I look for the MLD contact information. The MLD website “Contact” page (which is accessible only via a small link at the bottom of the home page that says “CONTACT,” emphasis original) has two buttons: one for “MyLymeData Support” and one for “Researchers.” If users click on the “MyLymeData Support” option, they must select one of five ambiguous subcategories, none of which directly address potential issues with data breaches or other negative consequences of data sharing. Overall, I am left concerned about a number of issues: Is revoking my data a truly simple process? If the “Contact” page does not offer an option that matches my concerns, where will I go to find additional information?
Conclusion
Unfortunately, nearly fifty years later, many of the problems articulated by the WATB authors remain unsolved. Many patients still do not receive necessary preventative care (183). Black women are three- to four-times more likely than white women to die in childbirth—unchanged from 1970 (183).5 As the authors lamented, children still lack sufficient vaccines and major cities are experiencing outbreaks of previously eradicated diseases (179). We have been unable to ameliorate the root causes of so many health problems: “bad housing, poor nutrition, poor sanitation, pollution, and dangerous working conditions” (179). It is still true that many of these issues are “suffered mainly by poor people who have no control over them” (179). And, perhaps worst of all, the U.S. still spends more money per person on healthcare than any other country (182).
Accordingly, feminist rhetoricians and healthcare activists are tasked with identifying “new forms of feminist knowledge that meet the challenges of corporatized, neoliberal health care” (Dubriwny 154). One of these challenges is figuring out who, specifically, health information sharing platforms aim to support. It is easy to imagine how health information sharing platforms would be different if average patient users had transformative user access to their research, data collection, and publication processes. In Kristin Arola’s book chapter, “Indigenous Interfaces,” she considers how Facebook would be different if it had been created “by and for” American Indian users (209). Drawing on interviews with twelve American Indian people, mostly from the Keweenaw Bay Indian Community Lake Superior Band of Chippewa Indians, Arola argues that a Facebook for American Indians would look different, perhaps using Native colors and “iconic image[s] like a feather or medicine wheel” (212). She also suggests that it would be used differently, in a way that “allows and encourages certain actions important to a group of people” (215).
What are the actions that are important to people with chronic, contested, and ambiguous illnesses? Building on Arola’s findings, health information sharing platforms could allow for transformative user access by taking the following steps:
- Allowing patients to publicly use and discuss their data.
- Discussing the benefits and limitations of using “big data” as a research method and explaining how the platform is truly doing “big data” differently than other companies and organizations, which may sell or misuse data.
- Making the FAQ and terms of service pages more user-centered. Ultimately, terms of service documents are legal documents that govern data use and misuse. Adding bolding, highlighting, and other forms of emphasis; eliminating legalese whenever possible; and providing context about why users have certain rights and not others would invite transformative access.
Most importantly, it is integral that average patient users can be intimately involved with managing the site, making changes based on evolutions in patients’ needs, and analyzing and publishing the results of data collection projects. Instead of emphasizing the simplicity of big data and avoiding discussions of the potential for data misuse, which are typically only addressed in terms of service documents to which users must agree before signing up, health information sharing platforms should be community-oriented. They should provide tools to help users mine through other users’ data and anecdotes. They should include supporting information that contextualizes conventional and radical treatments, thus integrating scientific and medical research alongside patients’ stories. They should provide talking points for discussing the data with different types of healthcare providers (such as primary care providers versus specialists) and have charts outlining potential responses, noting how a patient might proceed if their efforts to share data are rebuffed.
In a world without dependable texts like OBOS to ground patients’ research, feminist rhetoricians must continue investigating Dubriwny’s core questions, especially: How can we “recognize” the important work of apps, website, and health data sharing platforms in a way that presents a “critical stance” yet does not “unquestioningly embrace” them entirely (161)? There is much work to be done, and by considering issues of power, individuality, and simplicity in language and information design, feminist rhetoricians are equipped to lead the way.
Endnotes
- This article was updated in March 2020 in response to letters from LymeDisease.org/MyLymeData and Invitae. The author wishes to thank representatives of these organizations for their interest in her article. The author has updated this article in an effort to correct any potential misunderstandings about the work of LymeDisease.org/MyLymeData and Invitae Corporation. To most effectively define the goals and work of these organizations, the author has chosen to quote directly (rather than paraphrase) from their websites and recent correspondence, sometimes at greater length than is typical in peer-reviewed journal articles in rhetorical studies. [return to text]
- As I’ve written elsewhere, patients are forced to find, contextualize, and evaluate what I call “wildcard sources” in their quest for good health information. Wildcard sources typically include a range of scholarly and non-scholarly features, such as “personal testimonies, interpretations of scholarly research, plain language descriptions of complex diseases, reference lists, frequently asked questions sections, and descriptions of provider qualifications” (164). [return to text]
- WATB and OBOS have been critiqued for its focus on white, middle and upper-middle class women’s experiences. While they may not have transformed the healthcare system for women of color nor people with other multiply marginalized identifies, the manuals clearly “[call] attention to” gender, race, and class power dynamics (De Hertogh, Lane, and Ouellette 12). [return to text]
- The author is unsure if this is a spelling error or an acronym. [return to text]
- This statistic has been reported by multiple publication venues. For more information, see the CDC’s Pregnancy Mortality Surveillance System webpage. [return to text]
Works Cited
“About MyLymeData.” MyLymeData. Accessed 19 Feb. 2019.
Adams, Heather Brook. “The Feminist Work of Unsticking Shame: Affective Realignment in the 1973 Edition of Our Bodies, Ourselves.” Peitho 21.3 (2019): 580-598.
Arola, Kristin L. “Indigenous Interfaces.” Social Writing/Social Media: Publics, Presentations, and Pedagogies, edited by Douglas M. Walls and Stephanie Vie, The WAC Clearinghouse and University Press of Colorado, 2017, pp. 211-226.
Beck, Estee. “Sustaining Critical Literacies in the Digital Information Age: The Rhetoric of Sharing, Prosumerism, and Digital Algorithmic Surveillance.” Social Writing/Social Media: Publics, Presentations, and Pedagogies, edited by Douglas M. Walls and Stephanie Vie, The WAC Clearinghouse and University Press of Colorado, 2017, pp. 37-52.
“Board of Directors.” Lymedisease.org. Accessed 20 Feb. 2020.
Boston Women’s Health Collective. Women and Their Bodies. 1970.
Buchbinder, Mara. All in Your Head: Making Sense of Pediatric Pain. U of California Press, 2015.
“Data and Surveillance.” Centers for Disease Control and Prevention. Accessed 2 March 2020.
De Hertogh, Lori Beth. “Feminist Digital Research Methodology for Rhetoricians of Health and Medicine.” Journal of Business and Technical Communication 32.4 (2018): 480-503.
De Hertogh, Lori Beth, Liz Lane, and Jessica Ouellette. “‘Feminist Leanings:’ Tracing Technofeminist and Intersectional Practices and Values in Three Decades of Computers and Composition.” Computers and Composition 51 (2019): 4-13.
Doshi, Marissa J. “Barbies, Goddesses, and Entrepreneurs: Discourses of Gendered Digital Embodiment in Women’s Health Apps.” Women’s Studies in Communication 41.2 (2018): 183-203.
Drew, Debra, and Hilary Hewitt. “A Qualitative Approach to Understanding Patients’ Diagnosis of Lyme Disease.” Public Health Nursing 23.1 (2006): 20-26.
Grundy, Quinn, et al. “Data Sharing Practices of Medicines Related Apps and the Mobile Ecosystem: Traffic, Content, and Network Analysis.” BMJ 364 (2019): 1920. doi 10.1136/bmj.l920.
Hallenbeck, Sarah. Claiming the Bicycle: Women, Rhetoric, and Technology in Nineteenth-Century America. SIU Press, 2015.
“Home.” MyLymeData. Accessed 19 Feb. 2019.
Jack, Jordynn. “Leviathan and the Breast Pump: Toward an Embodied Rhetoric of Wearable Technology.” Rhetoric Society Quarterly 46.3 (2016): 207-221.
Johnson, Lorraine. Letter to Jen Wingard and Wendy Sharer. 23 January 2020.
—. “Re: Dissertation.” Received by Sarah Singer, 11 April 2017.
Johnson, Robert R. User-Centered Technology: A Rhetorical Theory for Computers and Other Mundane Artifacts. SUNY Press, 1998.
Hirsch, Annemarie G., et al. “Obstacles to Diagnosis and Treatment of Lyme Disease in the USA: A Qualitative Study.” BMJ Open 8.6 (2018): e021367. doi:10.1136/ bmjopen-2017-021367.
Martin, Chris J. “The Sharing Economy: A Pathway to Sustainability or a Nightmarish Form of Neoliberal Capitalism?.” Ecological Economics 121 (2016): 149-159.
“Patient Powered.” MyLymeData. Accessed 20 March 2020.
Rebman, Alison W., Soloski, Mark J., and John N. Aucott. “Sex and Gender Impact Lyme Disease Immunopathology, Diagnosis and Treatment.” Sex and Gender Differences in Infection and Treatments for Infectious Diseases, edited by Sabra L. Klein and Craig W. Roberts, Springer, 2015, pp. 337-360.
Relman, Arnold S. “The New Medical-Industrial Complex.” New England Journal of Medicine 303.17 (1980): 963-970.
Seigel, Marika. The Rhetoric of Pregnancy. University of Chicago Press, 2013.
Singer, Sarah Ann. “Embracing Wildcard Sources: Information Literacy in the Age of Internet Health.” College English 82.2 (2019): 152-172.
Turk, Siu P., et al. “Post-treatment Lyme Disease Symptoms Score: Developing a New Tool for Research.” PloS One 14.11 (2019): e0225012. doi:10.1371/journal.pone.0225012.
Wells, Susan. Our Bodies, Ourselves and the Work of Writing. Stanford University Press, 2010.
“Who We Are.” LymeDisease.org, https://www.lymedisease.org/about-lymedisease-org/. Accessed 20 March 2020.
Wormser, Gary P., et al. “The Clinical Assessment, Treatment, and Prevention of Lyme Disease, Human Granulocytic Anaplasmosis, and Babesiosis: Clinical Practice Guidelines by the Infectious Diseases Society of America.” Clinical Infectious Diseases, vol. 43, no. 9, 2006, pp. 1089-1134.